
HEALTH: When blood sugar spikes, the ultimate guide to hyperglycemia
Una glucosa alta no es solo un número en una pantalla. Es una señal que el cuerpo lleva demasiado tiempo intentando enviar, y aprender a escucharla a tiempo puede cambiarlo todo.
High blood sugar isn’t just a number on a screen. It’s a signal your body has been trying to send for far too long, and learning to listen to it in time can make all the difference.

La hiperglucemia afecta a cientos de millones de personas en el mundo, muchas sin saberlo. No es una enfermedad en sí misma, sino un aviso del organismo de que algo en su equilibrio interno está fallando. Entender qué la provoca, cómo se manifiesta y cuándo exige atención inmediata es hoy más fácil que nunca —y también más urgente— gracias a los nuevos datos y herramientas que la ciencia pone a nuestra disposición en 2026.
Hyperglycemia affects hundreds of millions of people worldwide, many without knowing it. It’s not a disease in itself, but rather a warning from the body that something is amiss in its internal balance. Understanding what causes it, how it manifests, and when it requires immediate attention is easier than ever—and also more urgent—thanks to the new data and tools that science will make available to us in 2026.
Qué ocurre realmente en el organismo / What really happens in the body
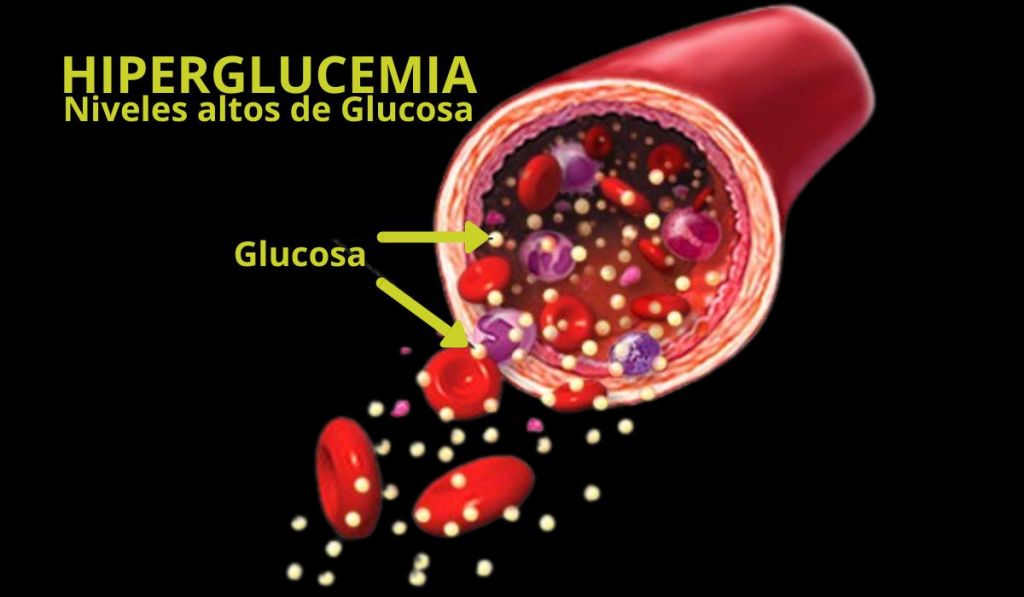
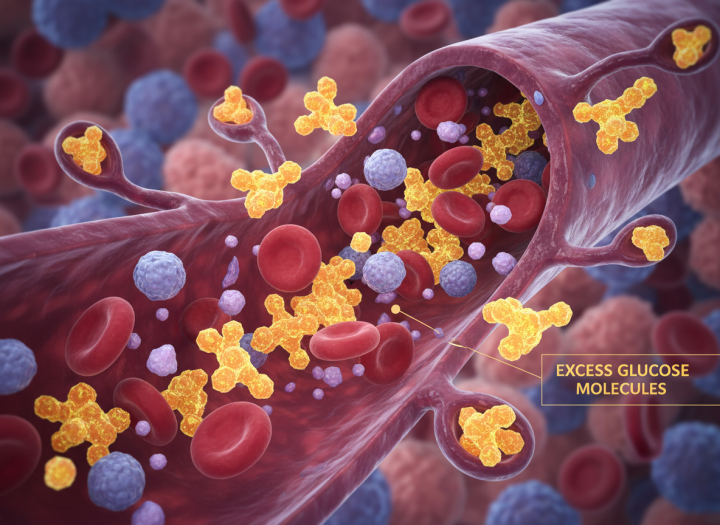
La glucosa es el combustible principal de cada célula. Cuando su concentración en sangre supera los valores que el cuerpo puede manejar con eficacia, hablamos de hiperglucemia. No aparece de golpe: es el resultado de un desequilibrio entre la cantidad de glucosa que circula y la capacidad del organismo —principalmente a través de la insulina— de utilizarla o almacenarla.
Glucose is the primary fuel for every cell. When its concentration in the blood exceeds the levels the body can effectively manage, we call it hyperglycemia. It doesn’t appear suddenly: it’s the result of an imbalance between the amount of glucose circulating and the body’s ability—primarily through insulin—to use or store it.
Ese desequilibrio puede deberse a la falta de insulina, a una resistencia creciente a su acción, a un aumento repentino de las necesidades metabólicas —como ocurre durante una infección o una cirugía— o al efecto de ciertos medicamentos. No es sinónimo de diabetes, aunque puede ser su primer aviso. Y no es sinónimo de cetoacidosis, aunque puede derivar en ella si no se actúa a tiempo.
This imbalance can be due to a lack of insulin, increasing resistance to its action, a sudden increase in metabolic demands—as occurs during an infection or surgery—or the effects of certain medications. It’s not synonymous with diabetes, although it can be its first warning sign. And it’s not synonymous with ketoacidosis, although it can lead to it if not addressed promptly.
Importante: Los cuerpos cetónicos no aparecen simplemente por tener la glucosa elevada. Se producen cuando hay un déficit significativo de insulina y el organismo empieza a quemar grasa como fuente de energía alternativa. Saber distinguirlo marca la diferencia entre una actuación domiciliaria y una urgencia hospitalaria.
Important: Ketone bodies don’t appear simply because of elevated glucose levels. They are produced when there is a significant insulin deficiency and the body begins to burn fat as an alternative energy source. Knowing how to distinguish between them makes the difference between managing the situation at home and requiring hospital emergency care.
Las causas más frecuentes —y las que más se pasan por alto / The most frequent causes — and the most overlooked
Las razones habituales son conocidas: olvidar una dosis de insulina o de antidiabéticos orales, comer más hidratos de lo previsto, reducir la actividad física o sufrir una infección. Lo que la medicina ha comenzado a destacar con más fuerza en los últimos años es la hiperglucemia inducida por medicamentos.
The usual reasons are well-known: forgetting a dose of insulin or oral antidiabetic medication, eating more carbohydrates than planned, reducing physical activity, or suffering from an infection. What medicine has begun to emphasize more strongly in recent years is drug-induced hyperglycemia.
Los glucocorticoides son los más reconocidos. Pero las guías ADA 2026 añaden una mirada específica a otros fármacos: estatinas, diuréticos tiazídicos y ciertos antirretrovirales también pueden elevar la glucosa, y ahora se recomienda explícitamente hacer seguimiento glucémico en cualquier persona que inicie este tipo de tratamientos. A esto se suma la vigilancia especial sobre los inhibidores SGLT2, que en situaciones concretas pueden provocar cetoacidosis con glucosa aparentemente normal —lo que se conoce como cetoacidosis euglucémica—, un cuadro que puede confundir incluso a profesionales experimentados.
Glucocorticoids are the most recognized. But the 2026 ADA guidelines add a specific focus on other drugs: statins, thiazide diuretics, and certain antiretrovirals can also raise glucose levels, and glycemic monitoring is now explicitly recommended for anyone starting these types of treatments. In addition, there is special attention to SGLT2 inhibitors, which in specific situations can cause ketoacidosis with seemingly normal glucose levels—known as euglycemic ketoacidosis—a condition that can confuse even experienced professionals.
Síntomas que merecen atención / Symptoms that deserve attention
En sus fases iniciales, la hiperglucemia es silenciosa o imitadora. La sed intensa, la necesidad de orinar con frecuencia, el hambre persistente, el cansancio sin causa aparente, la visión borrosa o la pérdida de peso involuntaria son señales que a menudo se atribuyen al estrés, al calor o al paso del tiempo. También pueden manifestarse como infecciones que se repiten o heridas que tardan más de lo habitual en cicatrizar.
In its initial stages, hyperglycemia is often silent or mimicking. Intense thirst, frequent urination, persistent hunger, unexplained fatigue, blurred vision, or unintentional weight loss are signs often attributed to stress, heat, or simply aging. It can also manifest as recurring infections or wounds that take longer than usual to heal.
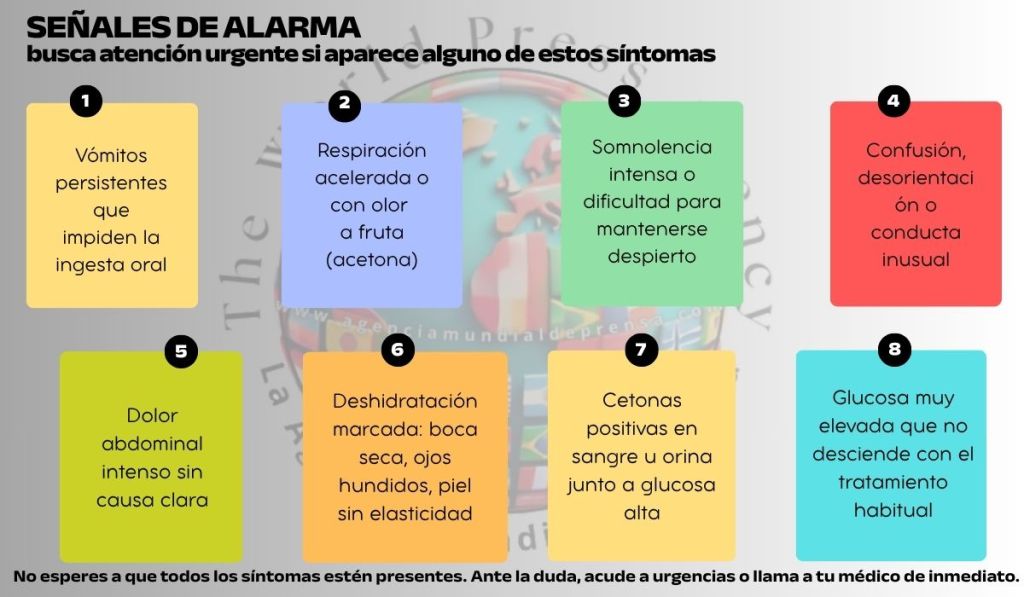
Cuando el cuadro progresa, el cuerpo ya no puede compensarlo: aparecen náuseas, vómitos, dolor abdominal, respiración acelerada, somnolencia y confusión. Esos síntomas ya no son compatibles con el manejo en casa. Obligan a descartar de inmediato una emergencia metabólica.
As the condition progresses, the body can no longer compensate: nausea, vomiting, abdominal pain, rapid breathing, drowsiness, and confusion appear. These symptoms are no longer manageable at home and require immediate evaluation to rule out a metabolic emergency.
Dos urgencias que no deben confundirse / Two emergencies that should not be confused
La cetoacidosis diabética y el estado hiperosmolar hiperglucémico son las dos complicaciones agudas más graves. Se parecen en que ambas requieren hospitalización y tratamiento urgente. Se diferencian en su mecanismo y en su presentación.
Diabetic ketoacidosis and hyperglycemic hyperosmolar state are the two most serious acute complications. They are similar in that both require hospitalization and urgent treatment. They differ in their mechanism and presentation.
La cetoacidosis se caracteriza por la presencia de cetosis y acidosis metabólica, y es más frecuente en diabetes tipo 1, aunque puede ocurrir en tipo 2. El estado hiperosmolar cursa con una hiperglucemia más pronunciada, deshidratación severa y ausencia o mínima presencia de cetosis; predomina en tipo 2, a menudo en personas mayores.
Ketoacidosis is characterized by the presence of ketosis and metabolic acidosis and is more common in type 1 diabetes, although it can occur in type 2. Hyperglycemic hyperosmolar state presents with more pronounced hyperglycemia, severe dehydration, and the absence or minimal presence of ketosis; it predominates in type 2 diabetes, often in older adults.
Novedad 2024: El consenso internacional actualizado recomienda medir el beta-hidroxibutirato de forma cuantitativa —idealmente en el propio punto de atención— en lugar de las tiras de cetonas en orina. Además, ahora se reconoce que algunos pacientes presentan cuadros mixtos, con componentes de ambas urgencias, algo más frecuente de lo que se pensaba. Las guías ADA 2026 incluyen tablas actualizadas de manejo para ambas entidades.
New for 2024: The updated international consensus recommends quantitative measurement of beta-hydroxybutyrate—ideally at the point of care—instead of using urine ketone strips. Furthermore, it is now recognized that some patients present with mixed symptoms, exhibiting components of both emergencies, which is more common than previously thought. The 2026 ADA guidelines include updated management tables for both conditions.
Cómo se trata hoy / How it is treated today
En una hiperglucemia sin descompensación aguda, las medidas son ordenadas y progresivas: revisar el tratamiento, ajustar la alimentación, identificar y corregir la causa desencadenante y reforzar el control glucémico bajo supervisión médica. Si la persona toma insulina, puede necesitar ajustar su pauta.
In cases of hyperglycemia without acute decompensation, the measures are systematic and progressive: review the treatment, adjust the diet, identify and correct the underlying cause, and reinforce glycemic control under medical supervision. If the person is taking insulin, their dosage may need adjusting.
En las urgencias —cetoacidosis o estado hiperosmolar— el tratamiento es hospitalario: reposición intensiva de líquidos, corrección de electrolitos, insulina intravenosa y tratamiento de la causa subyacente. La velocidad de actuación en estas situaciones es determinante.
In emergencies—ketoacidosis or hyperosmolar hyperglycemia—treatment is hospitalized: intensive fluid resuscitation, electrolyte correction, intravenous insulin, and treatment of the underlying cause. The speed of intervention in these situations is crucial.
Una novedad importante en 2026: los agonistas del receptor GLP-1, fármacos que ya han demostrado beneficios cardiovasculares y renales, se posicionan ahora como preferidos frente a la insulina en personas con diabetes tipo 2 sin hiperglucemia severa. Este cambio de paradigma refleja que el objetivo ya no es solo bajar la glucosa, sino proteger órganos.
An important development in 2026: GLP-1 receptor agonists, drugs that have already demonstrated cardiovascular and renal benefits, are now positioned as preferred alternatives to insulin in people with type 2 diabetes without severe hyperglycemia. This paradigm shift reflects that the goal is no longer just to lower glucose levels, but to protect organs.
La revolución silenciosa de la monitorización continua / The silent revolution of continuous monitoring
Si hay una transformación que define el manejo de la glucosa en 2026, es la consolidación de la monitorización continua de glucosa (MCG). Estos pequeños sensores, colocados bajo la piel, miden los niveles glucémicos cada pocos minutos y ofrecen algo que los análisis puntuales nunca pueden dar: el patrón completo. Tendencias, variabilidad, episodios nocturnos, respuesta a los alimentos.
If there’s one transformation that will define glucose management in 2026, it’s the consolidation of continuous glucose monitoring (CGM). These small sensors, placed under the skin, measure blood glucose levels every few minutes and offer something that spot tests can never provide: the complete picture. Trends, variability, nighttime episodes, response to food.
Las guías ADA 2026 dan un paso más y recomiendan que los sistemas de liberación automática de insulina se ofrezcan no solo a personas con diabetes tipo 1, sino también a quienes tienen diabetes tipo 2 en tratamiento con múltiples dosis de insulina. Además, se validan las métricas propias de la MCG —especialmente el «tiempo en rango», es decir, el porcentaje de horas en que la glucosa se mantiene entre 70 y 180 mg/dL— como objetivos terapéuticos primarios, al mismo nivel que la hemoglobina glicosilada.
The 2026 ADA guidelines go a step further and recommend that automatic insulin delivery systems be offered not only to people with type 1 diabetes, but also to those with type 2 diabetes treated with multiple daily insulin injections. Furthermore, CGM metrics—especially «time in range,» that is, the percentage of hours glucose remains between 70 and 180 mg/dL—are validated as primary therapeutic targets, on par with glycated hemoglobin (HbA1c).
Horizonte 2026: Investigadores del Center for Diabetes Technology de la Universidad de Virginia han demostrado que un algoritmo basado en MCG puede guiar el ajuste automático de insulina basal de forma tan eficaz como el método clásico de pinchazos capilares, reduciendo la carga del paciente y la inercia clínica. En el congreso ATTD celebrado en Barcelona en 2026, los sistemas de asa cerrada (páncreas artificial) se presentaron ya como herramientas consolidadas que reducen cetoacidosis, hipoglucemias graves y mejoran el tiempo en rango.
Horizon 2026: Researchers at the Center for Diabetes Technology at the University of Virginia have demonstrated that a CGM-based algorithm can guide the automatic adjustment of basal insulin as effectively as the traditional finger-prick method, reducing patient burden and clinical inertia. At the ATTD congress held in Barcelona in 2026, closed-loop systems (artificial pancreases) were presented as established tools that reduce ketoacidosis, severe hypoglycemia, and improve time in range.
La prevención empieza antes de que aparezca / Prevention begins before it appears
Las guías de 2026 recomiendan el cribado para prediabetes y diabetes tipo 2 a partir de los 35 años para toda la población, y en personas de cualquier edad con sobrepeso y al menos un factor de riesgo adicional. Detectar la hiperglucemia moderada —antes de que evolucione— sigue siendo la intervención más eficaz disponible.
The 2026 guidelines recommend screening for prediabetes and type 2 diabetes starting at age 35 for the entire population, and for overweight individuals of any age with at least one additional risk factor. Detecting moderate hyperglycemia—before it progresses—remains the most effective intervention available.
La educación diabetológica continúa siendo irreemplazable: saber cuándo medir la glucosa, cuándo revisar las cetonas, cómo actuar ante una enfermedad intercurrente y cuándo acudir con urgencia puede evitar una hospitalización. La tecnología amplifica esas decisiones, pero no las sustituye.
Diabetes education continues to be irreplaceable: knowing when to measure glucose, when to check ketones, how to manage an intercurrent illness, and when to seek urgent care can prevent hospitalization. Technology amplifies these decisions, but it does not replace them.
Descubre más desde LA AGENCIA MUNDIAL DE PRENSA
Suscríbete y recibe las últimas entradas en tu correo electrónico.
